Why Elder Care Franchise Is Becoming Cornerstone Healthcare
Elder care businesses used to be framed as lifestyle help. Now they’re increasingly treated like community-based clinical support that keeps the whole local healthcare ecosystem from gridlocking.
And this is where a reputable elder care franchise and franchising start to matter, because “cornerstone” doesn’t mean “helpful.” It means reliable, repeatable, and accountable.
Source: Pexels
Demographics Turned Elder Care into “Infrastructure,” not a Side Service
Picture a Tuesday discharge planner with three beds waiting, two families on speakerphone, and one stubborn reality: more people need help at home than the local system can “wing.” The aging curve isn’t a trend anymore; it’s a permanent operating condition.
The Congressional Budget Office’s demographic outlook for 2025–2055 makes the direction clear: the share and number of older adults rises materially over the coming decades, with direct implications for Medicare, Medicaid, and local capacity planning.
That shift changes where healthcare happens.
We’re watching the center of gravity move outward from hospital to home, from episodic treatment to ongoing support.
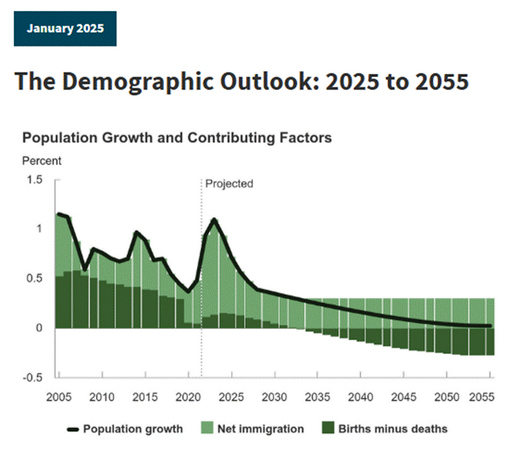
Source: CBO
A Franchise: A Compliance Engine With a Friendly Smile
Home-based elder care sits in a surprisingly legal-heavy intersection:
● consumer protection
● privacy
● labor law
● state licensing rules
● payer documentation
● Medicaid contracting requirements
The magic trick a strong franchise pulls off is simple: it turns that complexity into standard operating behavior, not heroic improvisation.
A good system pushes compliance into daily habits.
● How intake is documented, how care plans are updated, how incidents are escalated, how families are communicated with, how records are stored, how staff are screened, and how referrals are tracked. That’s not just “nice.” It’s risk containment.
In 2024, CMS finalized the Medicaid “Ensuring Access” rule, which directly touches fee-for-service, managed care, and home and community-based services (HCBS) with a focus on access, quality, and transparency.
The Hospital-to-Home Handoff is Now a Clinical Relay
Here’s the short narrative you’ve probably lived: a daughter drives her dad home after a fall. Discharge instructions are clear in theory, chaotic in practice. New meds, mobility limits, follow-up appointments, and a home that suddenly looks like a hazard course.
The hospital’s job is to stabilize. The community’s job is to sustain.
A mature elder care franchise becomes the local “relay runner” because it can deliver three things healthcare partners crave:
- Speed (start of care without weeks of confusion).
- Consistency (same protocols, same communication cadence, same escalation pathways).
- Receipts (documentation that stands up to payer and quality scrutiny).
This is also why payment policy changes matter even for non-medical care businesses.
CMS updates to Medicare home health payment rules and models reshape the incentives and pressures for home-based providers and their partners.
The CY 2025 Home Health PPS final rule is one example of how payment updates and policy refinements keep evolving, which ripples into referral patterns and how “home” is operationalized.
So, each section connects: demographics increase demand, regulation raises proof requirements, and the hospital-to-home relay forces organizations to perform like systems, not like solo operators.

Source: Pexels
The Staff: Your Biggest Liability and Your Biggest Differentiator
If elder care is becoming a cornerstone, the mortar is people. But the direct care workforce is under strain.
A Commonwealth Fund analysis highlights the scale of projected job growth in direct care and the challenge of meeting demand, even as home-based care becomes more common.
Franchises tend to do better here not because they have magic recruiting dust, but because they can standardize what reduces churn and incidents:
● Role clarity and scope boundaries so caregivers aren’t pressured into tasks that trigger safety or regulatory problems.
● Training that’s repeatable (especially around transfers, fall risk, dementia communication, and documentation).
● Supervision and escalation so “small issues” don’t become reportable events.
● Family expectation-setting so the care plan is realistic, and everyone knows what happens when conditions change.
Workforce connects back to compliance: the best legal defense is often a boring one, meaning you can show training logs, consistent policies, and documented follow-up.
Documentation and Tech are the New Bedside Manner
Elder care can’t become a healthcare cornerstone if it can’t speak healthcare’s language.
That language is notes, timestamps, care plans, incident reporting, and measurable follow-through.
The franchise advantage is the ability to implement one documentation standard across many homes and many caregivers, then build “translation” for partners: what information a hospital case manager needs, what a family needs, and what a payer expects.
This is also where the “human touch” paradox shows up: the warmer and more relational you are, the more you need structured communication so nobody relies on memory during stressful moments. The goal isn’t bureaucracy. It’s trust at scale.
Witty but useful rule: if it isn’t written down, it didn’t happen. If it’s written down poorly, it happened in court. Know the difference because it matters!

Source: Pexels
What to Look for in a Local Healthcare Cornerstone
This final section ties every “why” together into a practical checklist that reflects the demographic pressure, regulatory scrutiny, workforce reality, and care-transition demands discussed above.
Look for an elder care franchise that can clearly explain:
● How they define the scope of services (and what they refuse to do), with referral pathways for skilled needs.
● How they hire, screen, and train, and how often they retrain.
● How they document care, store records, and handle privacy expectations.
● How they handle incidents (falls, medication concerns, suspected abuse/neglect, sudden decline) with a clear escalation ladder.
● How they coordinate with local healthcare partners, including discharge planners and primary care offices, without overpromising.
● How they audit themselves: internal spot checks, caregiver supervision, client satisfaction tracking, and corrective actions.
Because the “cornerstone” claim is earned in the boring details.
When an elder care franchise gets those details right, it doesn’t just help families. It makes the local healthcare system work better: smoother discharges, fewer preventable crises, clearer accountability, and a safer home-based reality for people who are living longer and needing more support.